

FHIR vs HL7 for Payer Operations - The Compliance Reality Your Vendor Is Not Telling You

The market is flooded with 'FHIR-native' pitches. CMS-9115-F compliance deadlines are circled in red. And HL7 v2 pipelines are still doing exactly what they have always done moving eligibility files, ADT feeds, and claims at scale. The real question is not which standard wins. In this article, we'll go over what FHIR and HL7 v2 each handle, what CM]=” mandates require, and how to prepare.
FHIR Does Not Replace HL7 v2 in Payer Operations
Why This Distinction Matters Before Signing a Vendor Contract
A 2023 ONC survey found that 96% of health information exchanges still receive HL7 v2 ADT messages. Before any contract signature, demand an integration map showing exactly which workflows run on HL7 v2 and X12 and which run on FHIR. If a vendor cannot produce that map, the hidden integration work lands on the payer.
What FHIR-Native Actually Means vs. What It Means in a Sales Deck
Any system that exposes FHIR APIs can call itself FHIR-capable. That is a low bar. Truly FHIR-native means the internal data model is built around FHIR resources, not a relational EDI database with JSON bolted on the front. The difference surfaces at audit time, when a CMS reviewer requires conformant USCDI data from the Patient Access API. Ask the vendor to draw their data architecture showing HL7 v2, X12, and FHIR side by side. Vague answers to specific questions are answers.
The Payer Workflows That Remain HL7 v2 and X12 EDI-Dependent
Claims submission runs on X12 837. Remittance advice on X12 835. Enrollment on X12 834. Eligibility on 270/271. Hospital ADT feeds for census and STARS post-discharge tracking still flow through HIEs in HL7 v2.x format. CMS has not mandated FHIR for any of these transaction types, and the operational complexity of replacing them across thousands of provider and clearinghouse relationships is not on the near-term roadmap for anyone.
The Workflows Where FHIR R4 Is Now a Federal Mandate
CMS-9115-F and CMS-0057-F are explicit
- Patient Access APIs
- Provider Directory APIs
- Prior Authorization APIs
- Payer-to-Payer exchange must run on FHIR R4
Automating prior authorization alone is projected to save the healthcare industry up to $15 billion per year which explains why CMS is holding firm on the timeline. The X12 837 pipeline and the FHIR Patient Access API will run in parallel. Neither replaces the other.
What CMS Actually Requires and When
CMS-9115-F and CMS-0057-F Obligations Broken Down by Function and Deadline
Provider Directory APIs were required by January 1, 2021. Patient Access APIs went live for Medicare Advantage (MA) in January 2023 requiring adjudicated claims and encounter data dating back to January 1, 2016 with Medicaid and CHIP following by 2024.
Three requirements converge on January 1, 2026 with some enforcement grace through 2027:
- The Prior Authorization API
- The Provider Access API
- Payer-to-Payer data exchange
These are not aspirational targets. Noncompliance affects plan ratings and creates civil monetary penalty exposure.
Why Prior Authorization Is the Most Urgent Forcing Function for Regional Payers
The existing PA workflow likely involves proprietary portals, fax-based submissions, or X12 278 transactions. The Da Vinci PAS implementation guide requires a FHIR-based API that receives structured electronic PA requests and returns structured responses with defined turnaround time requirements. For most regional payers, this is a workflow redesign, not a UI update. Most internal UM systems were not built to emit or consume FHIR R4 resources natively, which means a translation and orchestration layer is almost certainly in the near-term roadmap.
Payer-to-Payer Data Exchange Requirements and What They Expose
When a member switches plans, the losing payer must share up to five years of clinical data formatted as USCDI v1 FHIR resources with the gaining payer. The receiving payer must then ingest that data and expose it through all of its own APIs. That chain breaks at the EMPI. To respond correctly, the payer must match the incoming member request to a record in the system, pull the appropriate history, translate it into conformant FHIR resources, and return it through a working API. Fragmented member identity makes all of that unreliable.
Where HTI-5 Fits in the CMS-9115-F Compliance Picture
ONC's HTI-5 rulemaking extends FHIR-based interoperability into clinical decision support and algorithmic transparency. For payers with UM tools that use predictive models to inform PA decisions, HTI-5 creates disclosure obligations that intersect with the FHIR API architecture. If the platform produces PA decisions that will need to be explainable under HTI-5, the data trail for those decisions must be structured and accessible. Da Vinci CDex is one mechanism for that. It belongs in compliance planning alongside CMS-9115-F.
Da Vinci Implementation Guides
Why Da Vinci Matters More Than Generic FHIR R4 Compliance for Payers
Generic FHIR R4 compliance means a system can produce and consume FHIR-formatted resources per the base spec. The Da Vinci Project, an HL7 FHIR Accelerator initiative, produces payer-specific implementation guides that define exactly how prior authorization, clinical documentation exchange, and coverage requirements should work in FHIR. CMS references Da Vinci IGs by name in its rulemaking. A vendor claiming FHIR R4 compliance without Da Vinci IG support is selling infrastructure without workflow logic.
PAS, CDex, and CRD Implementation Guides
PAS, the Prior Authorization Support guide, defines how PA requests and responses flow between providers and payers in FHIR R4. It is what CMS-0057-F mandates for January 2026.
CDex, the Clinical Data Exchange guide, defines how payers request structured clinical documentation from provider EHRs to support risk adjustment, quality reporting, and audits.
Coverage Requirements Discovery (CRD) gives providers real-time access to payer authorization requirements at the point of care, moving the PA check upstream before a service is ordered. The Payer Coverage Decision Exchange (PCDE) IG handles the transfer of active treatment plans and coverage decisions during plan transitions, preventing care gaps when members switch plans.
How Da Vinci PAS Maps onto the Existing Prior Authorization Workflow
The current PA workflow involves a provider submission, a UM review against clinical criteria, and a decision back through the same channel. Da Vinci PAS replaces the submission and response channel with a structured FHIR API exchange. The clinical review logic does not change. What changes is the intake and output format and the requirement that the decision be returned as a machine-readable FHIR response the provider's EHR can consume directly. Most UM platforms need either a PAS-native replacement or an integration layer that handles FHIR translation without degrading the decision audit trail.
What to Ask the Vendor Before Accepting FHIR-Compliant as a Complete Answer
Four questions every payer CIO should require clear answers are:
- Which Da Vinci IGs does the platform support, and at what version?
- Is Da Vinci PAS support native or a translation layer over a proprietary PA workflow?
- How does the platform handle HL7 v2 and X12 EDI ingest alongside FHIR, and where does the translation occur?
- Can the vendor demonstrate passing a Da Vinci Connectathon or reference a conformance testing toolkit?
Vague answers mean the hard integration work falls on the payer.
Running HL7 v2 and FHIR in Parallel
Why Mature Payer Data Architectures Will Operate Both Standards for the Foreseeable Future
There is no realistic near-term scenario in which a regional payer or Medicare Advantage organization shuts off HL7 v2 and X12 EDI. The transaction volumes, provider relationships, clearinghouse agreements, and CMS reporting requirements that depend on those standards are not going anywhere. What is happening is that FHIR R4 APIs are being added on top of existing infrastructure. The teams that architect this well end up with a more capable platform. The teams that bolt FHIR on without rationalizing the underlying data model end up with a more expensive, more fragile one.
The Translation and Orchestration Layer Challenge
When an HL7 v2 ADT message arrives from an HIE and a FHIR Patient resource arrives from a Payer-to-Payer exchange describing what appears to be the same member, something has to reconcile them.
What the Translation and Orchestration Layer Parses
- V2 segments
- Extracts FHIR JSON
- Maps both to the internal data model,
- Resolves them against the EMPI
- Routes the result downstream
This is not a connector problem. It is an architecture problem. The layer has to handle schema evolution in both standards, FHIR profile version differences, and the quirks of individual payer and HIE implementations that do not always follow the spec precisely.
How FHIR JSON Resources Land Alongside HL7 v2 and X12 EDI in Snowflake and Databricks
Modern payer data warehouses on Snowflake or Databricks can hold both HL7 v2 parsed data and FHIR JSON natively. Snowflake's VARIANT column and Databricks Delta Lake support querying FHIR resources with SQL without full schema normalization upfront. The hard part is consistency: when an HL7 v2 claim update reflects a V28 diagnosis change, that change must propagate to the FHIR data store. A CDC or message queue process handling that propagation is not optional. It is table stakes for a dual-standard architecture.
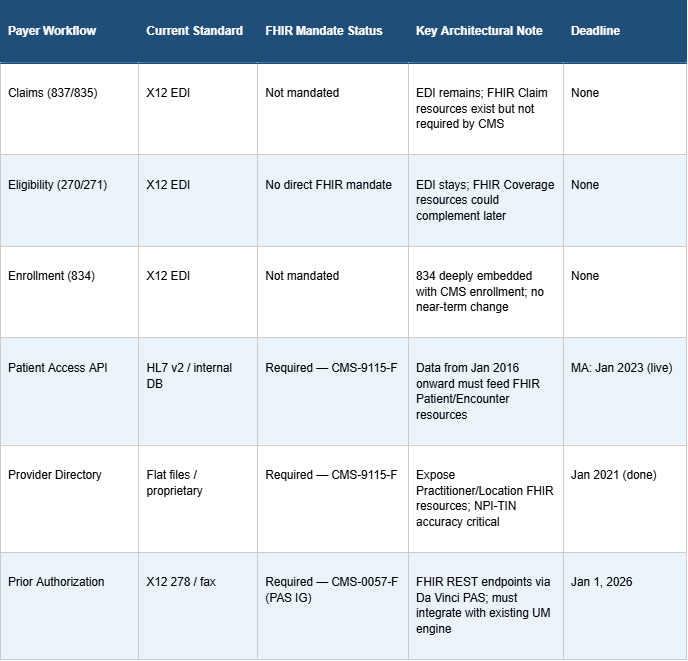
Payer Use Case Comparison
The table below maps current payer workflows to their current standard, FHIR mandate status, and key architectural notes. Use it as a starting point for vendor briefings and internal planning sessions.
What Regional Payers Should Actually Do with This Information
FHIR as a Checkbox API Layer vs. FHIR as a Member Data Foundation Rebuild
Two approaches exist. The first is building the minimum API surface required to satisfy CMS-9115-F and CMS-0057-F, passing the audit, and moving on. The second is using the FHIR mandate as a forcing function to resolve EMPI fragmentation and build a data model that supports risk adjustment, quality reporting, and care management on a more coherent foundation.
The first approach costs less upfront and more over five years. Every FHIR API bolted onto a fragmented data model creates technical debt that compounds with each new mandate.
Which Payer Organizations Will Extract Revenue from FHIR Compliance
The payers that turn FHIR compliance into a revenue story are the ones that connect the following:
- CDex to their risk adjustment engine
- CRD to their care management workflows
- Payer-to-Payer exchange to a clean EMPI
A well-architected CDex implementation is a risk adjustment tool. A well-architected CRD implementation reduces unnecessary PA friction, which improves provider satisfaction, which ultimately affects STARS measures tied to member experience. Checkbox payers spend the compliance budget and see no return. Architecturally serious payers generate measurable revenue from the same investment.
Practical Next Steps for a CIO Beginning a FHIR Readiness Assessment
Start with a workflow inventory. Document which systems produce and consume each HL7 v2 and X12 transaction type, and identify where translation layers already exist. Map CMS-9115-F and CMS-0057-F obligations against that inventory to find the gaps. Run an EMPI audit in parallel the percentage of member records with confident identity matches across eligibility, claims, and clinical data indicates how much remediation work remains before a reliable Payer-to-Payer exchange is achievable. Then evaluate vendors against a Da Vinci IG checklist PAS, CDex, CRD not generic FHIR R4 claims. Engage with HL7 Da Vinci Roundtables where payers share real implementation lessons. The teams that ask the right questions before contracts are signed build less technical debt and more operational leverage from the compliance work they have to do regardless.
Final Thoughts
The compliance obligations under CMS-9115-F and CMS-0057-F are real, the January 2026 deadlines are firm, and the architecture challenge is not about picking a winner between two standards. It is about building a data environment that handles both without fracturing the member identity model or duplicating existing infrastructure.
The payers that come out ahead will use this compliance moment to strengthen their data foundation. Honest EMPI remediation, operationally specific Da Vinci IG support, and a parallel architecture strategy that lets HL7 v2 and FHIR coexist cleanly those decisions will separate the plans that extract revenue from FHIR compliance from the ones that merely survive it.
FAQs
How can Invene help payers navigate FHIR and HL7 compliance?
Invene is a healthcare technology firm that specializes in FHIR and HL7 interoperability for payers. We help regional health plans assess compliance gaps, design dual-stack HL7 v2 and FHIR architectures, and implement Da Vinci implementation guides including PAS, CDex, and CRD. For organizations preparing for CMS-9115-F deadlines or evaluating vendor contracts, Invene provides the technical depth and payer-specific expertise to move from compliance checkbox to operational advantage.
Is HL7 v2 being phased out in payer operations?
Not in any timeline relevant to current planning. A 2023 ONC survey found 96% of HIEs still receive HL7 v2 ADT messages. CMS has mandated FHIR R4 only for specific API use cases: patient access, provider directory, prior authorization, and payer-to-payer exchange. Claims, eligibility, and enrollment transactions remain on X12 EDI with no announced retirement date.
What is the difference between Da Vinci compliance and generic FHIR R4 compliance?
Generic FHIR R4 compliance means a system can produce and consume FHIR-formatted resources per the base spec. Da Vinci compliance means a system implements the payer-specific IGs PAS for prior authorization, CDex for clinical documentation exchange, CRD for coverage requirements discovery, and PCDE for payer-to-payer treatment continuity. CMS-0057-F references Da Vinci IGs by name, making them the operationally required standard.
What exactly is required by the January 2026 prior authorization deadline?
Impacted payers Medicare Advantage, Medicaid, CHIP, and QHP issuers on the FFE must implement FHIR R4 prior authorization APIs aligned to the Da Vinci PAS implementation guide by January 1, 2026, with some enforcement grace through 2027. The APIs must receive structured PA requests and return structured decisions with defined turnaround time requirements. CMS will also require payers to publish prior auth performance metrics for CY2025 by mid-2026.
Why does FHIR migration expose EMPI problems specifically?
FHIR Patient Access and Payer-to-Payer APIs require complete, accurate aggregation of member data across all source systems in response to API requests. That aggregation depends on an EMPI resolving identity consistently. Most payer architectures carry EMPI fragmentation from system acquisitions and plan migrations. FHIR API go-live surfaces that fragmentation as response quality failures that were previously invisible inside batch file processes.
Can a FHIR investment actually improve risk adjustment revenue?
Yes, when the architecture connects CDex to the right workflows. Da Vinci CDex allows payers to request structured clinical documentation from provider EHRs, which becomes a mechanism for confirming suspect HCCs identified through historical data or predictive analytics. Faster, more accurate HCC closure translates to higher RAF scores and increased CMS revenue per member per month. The compliance investment and the revenue opportunity are the same architectural decision.

James founded Invene with a 20-year plan to build the world's leading partner for healthcare innovation. A Forbes Next 1000 honoree, James specializes in helping mid-market and enterprise healthcare companies build AI-driven solutions with measurable PnL impact. Under his leadership, Invene has worked with 20 of the Fortune 100, achieved 22 FDA clearances, and launched over 400 products for their clients. James is known for driving results at the intersection of technology, healthcare, and business.
Ready to Tackle Your Hardest Data and Product Challenges?
We can accelerate your goals and drive measurable results.